1080 MAP as a quantitative and qualitative tool in the rehabilitation of a high level triathlete with low back and shoulder pain
Eriksrud, O., Parnevik-Muth, J., Ghelem, A. 1,2
1 Athletic 1080 AB, Stockholm, Sweden
2 1080 Motion AB, Stockholm, Sweden
Introduction
One reason why athletes and patients come to rehabilitation is to decrease pain and dysfunction, and to enhance physical performance. Any functional performance is dependent upon the interaction of mobility of different joints. Global movements, where subject engage the entire kinematic chain, will quantify total movement, or output of the body. One part of 1080 Movement Assessment Profile (1080 MAP) is based upon the unique combination of upper extremity reaches in different directions either measured in centimeters or degrees. Performance on these different global movements will give indications as to what joint(s) or region(s) to target in an intervention that is based upon movement and not symptoms. Furthermore, 1080 MAP can also guide combinations of movements to be used in treatment. The quantitative component of 1080 MAP does not say anything about the quality of the movement. The addition of qualitative assessment to the quantitative measures will provide further information as to what joints and regions to target in follow-up testing and treatment. The purpose of this case study is to investigate the effectiveness of the quantitative and qualitative components of 1080 MAP in guiding treatments for a high level triathlete with low back and shoulder pain.
Subject description
VL is a 35 years old male triathlete with long-standing low back and right shoulder pain. He is training about 15 hours a week, alternating biking, swimming and running. He came for therapy November 2013. His major goal was to decrease pain to enable effective training and enhance performance.
Examination
Pain was associated with the following movements: when performing a motion the mimics the freestyle arms stroke (shoulder flexion and internal rotation) with the right arm. VL could not run without low back pain. He rated both his right shoulder and low back pain 5/10 on 0-10 scale. Mobility and stability was evaluated bilaterally using 1080 MAP to quantify global movement and guide further testing. 1080 MAP standing on the right foot (score: 7.2) is presented in Figure 1 below.
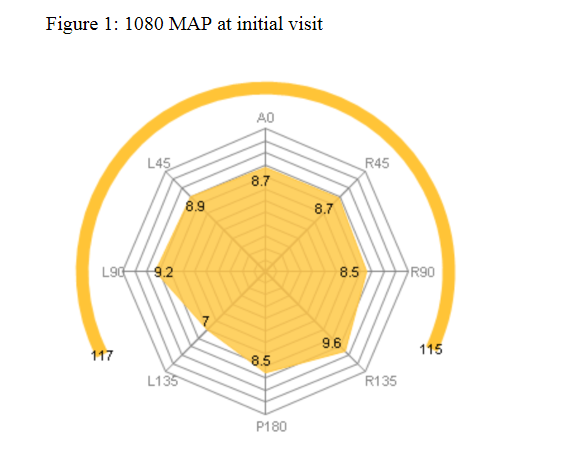
The quantitative profile was evaluated with the conclusion that the patient had an overall good global mobility and stability. However, based upon further qualitative and quantitative analyses, limitations were found standing on the right foot and reaching with his right arm. This was especially true in the L135 direction. This led to further testing of the right midfoot, right hip internal rotation, right thoracic rotation, scapulothoracic articulation and left cervical rotation. The results were as follows: • Right midfoot: 1/5 inferior glide of talus on navicular bone • Right hip internal rotation: 25 degrees • Right thoracic rotation: 30 degrees • Scapulothoracic mobility testing: soft tissue restrictions limiting medial glide (serratus anterior) with lattisimus dorsi tightness. • R shoulder: 2/5 inferior glide
Intervention
Manual treatment was implemented in the early stages in order facilitate mobility of the restrictions identified in the right midfoot, hip, thoracic spine as well as scapulothoracic articulation. All mobilizations for joint mobility were followed by stability exercises for the same motions in the different joints and regions. During the initial visit we also scheduled a Vo2max test to test for running economy. He completed his test with a measure of 58ml/kg/min. VL was given 4 exercises to do on his own that was done twice a day for the first 4 weeks and then 3-4 times a week. For the decreased motion in the thoracic spine and the tightness of the right serratus anterior muscle he was given an exercise in left side lying reaching back and up with his right arm with thoracic spine rotation to the right. He was also given a lattisimus dorsi stretch in standing, a hip stretch on the floor to increase hip range of motion, and a mobility and stability exercise in standing holding a 3 kg free weight in each hand reaching with the arms and opposite foot in all three planes of motion. VL came to therapy a total of five times, after which he felt more flexible and no low back or shoulder pain. He was scheduled to come back for re-test after Masters SM in 800 m freestyle 3 months later to evaluate if he had been able to keep himself pain free and to see if his mobility and stability had improved.
Outcome
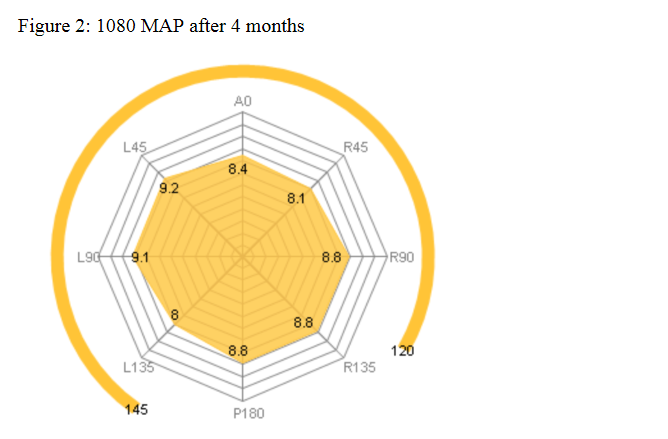
After three months and five physical therapy sessions the same 1080 MAP profile was performed on the right foot with a score of 7,7 (Figure 2), which is a 7% increase. As we can see from this profile the reach mostly targeted as important, L135, was improved by 14%. However, there was also a decrease in performance on some of the other reaches. He pain level was at this point also reported to be 0/10 in the shoulder and low back with activity.
• Right midfoot: 3/5 inferior glide of talus on navicular bone • Right hip internal rotation: 40 degrees • Right thoracic rotation: 40 degrees • Scapulothoracic mobility testing: Minimal tightness of the serratus anterior and the lattisimus dorsi. The quality of movement improved. With the increased mobility in the right foot and hip he was able to use his hips instead of his back when reaching back overhead along the L135 and P 180 vector. With the scapula in a better position due to decreased serratus anterior tightness and the increased flexibility in the lattisimus dorsi he was able to reach overhead without right shoulder impingement. Patient was scheduled for a new V02 max with a lactate profile after 6 weeks to see the immediate effects of improved mobility and stability on movement efficiency. However, this was obtained due to patient being sick at the time of the test and failure to reschedule. This result is therefore not reported. VT won silver in 800 freestyle Masters SM in Sundsvall, which is a career best. He is now able to swim, run and bike without pain.
Discussion
VT made great improvements in being able to train and compete without pain, and reports a greater freedom in moving in both training and competition. The 1080 MAP profile did show an overall improvement in terms of area and symmetry on the right foot, however not all reaches improved. This lack of quantitative improvement can be explained by a change in the quality of the movement. This shows why it might be important to have a qualitative measure integrated with the quantitative in the 1080 MAP profile. Furthermore, it was unfortunate that a VO2max test and lactate profile could not be included to evaluate if mobility and stability had an influence on running economy after 6 weeks. The short time interval here was selected to avoid other training effects. In conclusion this case study shows how 1080 MAP can be a systematic and effective tool in both the quantitative and qualitative assessment of overall movement that can guide follow-up tests and treatment.