Whether caused by swinging a racket, bat, or club, an internal oblique tear presents rehab professionals with a particular challenge: How do you set return-to-play protocols for an injury caused by the exact movement which needs to be rehabilitated in order to resume play?
Impacting the core abdominal muscles used in rotational sports, oblique strains and tears routinely immobilize football quarterbacks, baseball hitters, golfers, and tennis pros. Speaking with MLB.com’s Lindsey Berra in 2017, LA Dodgers Athletic Trainer Stan Conte traced a rise in oblique injuries in Major League Baseball to the increased focus on year-round strength training, with players escalating their explosive power and increasing the force that travels through the kinetic chain.
“If that oblique isn’t strong enough to handle the force from the legs,” said Conte, a specialist and researcher who also operates Conte Injury Analytics, “It gives.”
An Alternative Approach
Shut it down. Rest. Give it a few weeks, maybe longer. Depending on the severity of the strain or tear, the common prescription for an oblique injury is to put athletic activity entirely on hold. Under normal circumstances, convincing driven athletes to rest can be a challenging task, but an oblique tear doesn’t merely compromise performance—since the injury subjects daily actions like laughing, coughing, or sliding into a car seat to a sudden explosion of excruciating pain, athletes may be more than willing to skip a few workouts.
At times in the competitive cycle, however, those same athletes may not have the luxury of taking a month off of training and then laboring to regain competition readiness from there.
“One of the most difficult hurdles returning to sport following injury is maintaining conditioning to perform against competition,” says Adam Rolf, a physical therapist and performance specialist with 13 years of experience in the field. “This loss of conditioning leads to decreased performance when returning to sport.
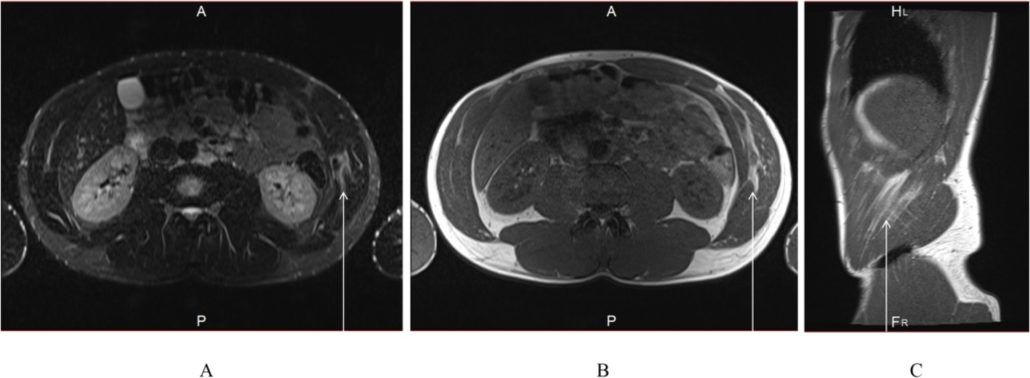
2016. The French Open a mere month and a half away on the calendar. Pro tennis player Robert Lindstedt suffered a tear of the left internal abdominal oblique while delivering a serve during a tournament match in Turkey.
“Ten years ago, for this type of injury I would have had to refer out [to a specialist] and cross my fingers,” offers Ali Ghelem, Lindstedt’s longtime trainer. “For me, it would be impossible to tell him you are okay to go or not. And he might have tried to manage the pain with painkillers and tried to play anyway—as soon as he could hit the ball, he would go.”
And, by rushing back to the court, the athlete would likely to be at a significant risk for re-injury. Studying two decades of abdominal strains in the MLB, Stan Conte not only found that the incidence of oblique strains had been increasing over that span, but also that the re-injury rate was a relatively high 12.1%.
“It’s very hard to isolate this area and send force through it without actually re-injuring yourself,” concedes Ghelem.
In Lindstedt’s case, Ghelem began the rehab process immediately (read the full Case Study by Ola Eriksrud, Ali Ghelem, and Jan Cabri published by Physical Therapy in Sport here). Just days after the injury, using the 1080 Quantum, Ghelem programmed a sequence of isokinetic exercises that included a bilateral rotational pull, unilateral vertical press, and unilateral anterior push. For these movements, Ghelem directed the athlete to exert force up until reaching a self-reported pain limit of 4 on a scale of 10.
Setting an athlete-controlled “speed limit” on the cable machine, Ghelem provided Lindstedt the ability to manage the load of each rep and each set of every movement, empowering him to go harder during the parts of a movement where his body allowed it, and enabling him to naturally back off when the pain level crossed an established threshold.
The results of those early sessions? Lindstedt still reported pain in the injured area while performing the exercises, and was very concerned about his ability to compete in the upcoming Grand Slam events on his schedule.
However… while working with the speed limit on the Quantum, though he continued to experience a self-reported pain level of 4 during the course of the movements, just three days after his first rehab session he was able to exert 50-100% more force on the movements he controlled.
That injured oblique was getting stronger.
First, Do No Harm
“If you have a partial tear and you swing aggressively, it can get worse,” said Dr. Ara Suppiah on the Golf Channel, discussing the 2018 oblique injury that threated to keep pro golfer Rickie Fowler from competing in the Ryder Cup. “More importantly, it alters the dynamics of the swing and you develop compensations, so you might start off with an injury here and end up tweaking your back or tweaking your hip, because it’s really a key component of the swing.”
Dr. Suppiah’s hypothetical prescription for Fowler? 2-3 weeks of rest. Which, it turns out, was similar to the course the big-hitting golfer ultimately followed, missing two playoff events in order to make a September return to assume his spot on the U.S. Ryder Cup team.
“Following injury, every opportunity to provide treatment matters when returning to play at a major event. Our job is to provide the athlete the clearest path back utilizing best practice techniques to improve pain, regain strength and increase fitness,” offers Adam Rolf, who is also an NSCA Conditioning certified Strength and Conditioning Specialist (CSCS) and credentialed as a Titleist Performance Golf Fitness Instructor (CGFI).
“Successful return to game readiness is heavily based on the ability of the athlete and therapist to communicate well through the process,” Rolf continues. “For example, providing resistance training with Quantum allows real-time objective feedback optimizing each session’s training intervention effectiveness.”
Preparing Lindstedt to return to high level competition after his oblique tear, Ghelem could be confident in his ability to progress the athlete in the safest, most efficient, and most effective manner possible.
“Because you’re loading optimally all the time, you can do less work in terms of volume. And if you do less volume, the recovery time between sessions is going to be short also. So you actually can go higher intensity with the loading, but with less volume and stimulate that recovery process,” Ghelem says.
Had he lacked the ability to optimize his sessions in the same way, Ghelem admits that he would have had to take a more conservative approach, sacrificing competitive readiness to insure safety.
“[Without the Quantum] you have to undertrain, because you can’t change the load every three milliseconds on a normal weight stack. Or, if you take a normal cable machine, and you choose which weight the athlete is going to do and tell him to do eight reps, that’s pretty much impossible. You have to go so safe that you’re sure you’re not going to re-injure it right away.”
Return to Perform
“He felt in total control, and the fact that the numbers went up pretty much every session, and his pain level was the same, that told him he was healing at a good pace,” Ghelem says. “By the end of the process, he was able to push harder and harder, and eventually the last sessions he could push 100%. But he was not strong enough yet.”
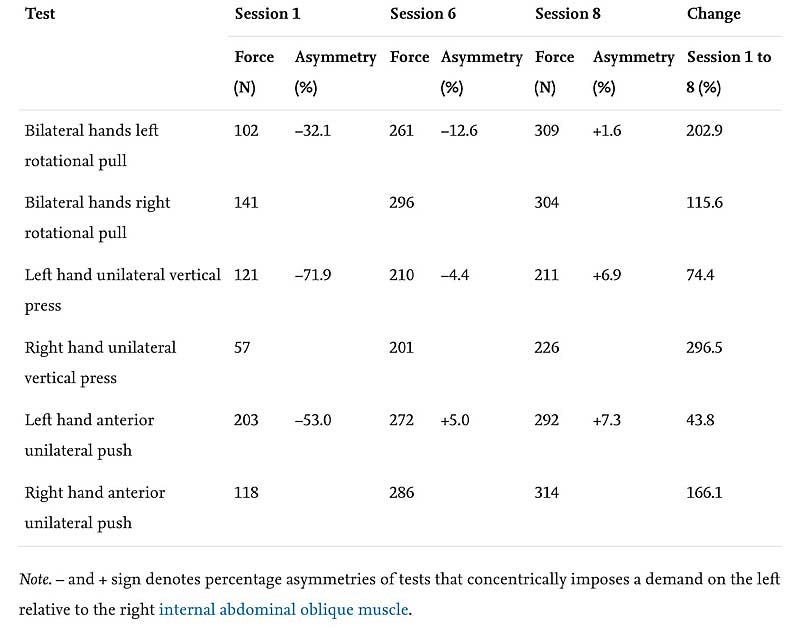
The established return to sport criteria proved to be important at session six since there was no pain during any of the exercises, but there were asymmetrical force measurements ranging from −12.6 to +5.0%. During this session both the coach and the player agreed that return to competition should be postponed based on the force symmetry criteria, and that the player felt apprehensive in attempting to serve. Then, at session eight, when the player returned to sport, no mean force deficits were observed and the player was more confident in the serve. (Eriksrud, Ghelem, & Cabri).
In this case, Ghelem used the force data provided by the Quantum to show his athlete that he was close… but not quite ready to perform at his goal event, The French Open, without risk of re-injury. Wimbledon was right around the corner, and rather than jumping back onto the court too early, Lindstedt continued his return-to-play efforts.
“When he was back to 100% on both sides, he started to train in tennis,” Ghelem says. “Then he had a couple of weeks and could play Wimbledon no problem, and he’s been playing for three years without re-injury.”