For athletes at any level, serious injuries can not only derail their progress in the sport, but also threaten a core part of their identity. This reality equally extends to adults who may not participate in a professional competitive sport. In most cases, at our clinic Therapie Kreuzplatz in Zurich, we are managing non-professional clients who nonetheless still play volleyball, soccer, or hockey, enjoy mountaineering and skiing, or those who join amateur leagues, enter weekend “fun runs,” and play recreationally.
With this population, among the biggest challenges we face is the return-to-participation process, including return-to-sport testing. Imagine a 40-year-old female recovering from ACL surgery who wants to resume playing volleyball twice a week with minimal risk of re-injury…but also has little-to-no formal background in strength training. If this were a 25-year-old elite pro volleyball player, we could follow and expand on established processes, but in this case, we have this gap we assume exists. Therefore, we have asked ourselves:
- 1. How do you utilize return-to-sport protocols developed for elite athletes when working with athletes who have little to no formal background in strength training?
- 2. How do we target the misdirection of hop tests in elite and recreational using the 1080 Quantum?
Regarding the high re-injury rate after ACL reconstruction in professional sports, return-to-sport (RTS) protocols have been questioned recently. Most likely, more return-to-participation decisions are made outside of the professional sports world. In this regard current protocols are partially easy to apply, like the timed hop, single hop, triple hop, and cross-over hop test, compared to maximal strength testing and the necessary equipment needed. However, besides its applicability, there are several barriers:
- A. The patient’s physical readiness for testing safely.
- B. Lack of personal responsibility to work on their strength deficits.
- C. Lack of support from insurance companies.
Consequently, in non-professional athletes, we are unfortunately very often confronted with no—or insufficient—clearance for RTS.
However, in professional athletes, insufficient clearance for RTS is also common and could be even higher when referring to the RTS definition from a consensus statement 2020:
“RTS is characterized by achieving the preinjury level of sports participation as defined by the same type, frequency, and QUALITY of performance as before injury.”
When we stick to the way we have approached this problem for years, trying to increase the number of people reaching LSI scores > 90%, we disregard the quality aspect of this definition. In the end, all groups are suffering from reinjuries or lasting pain, even though to a different degree; and it is usually justified by the insufficient clearance, which is mainly the performance score (LSI > 90%).
[av_button_big label=’More physical therapy and return-to-play:’ description_pos=’below’ link=’manually, https://1080motion.com/applying-1080-quantum-clinical-setting/’ link_target=” icon_select=’no’ icon=’ue800′ font=’entypo-fontello’ custom_font=’#ffffff’ color=’theme-color’ custom_bg=’#444444′ color_hover=’theme-color-subtle’ custom_bg_hover=’#444444′ av_uid=’av-154cfr9′]To Heal and To Correct: Applying the 1080 Quantum in a Clinical Setting [/av_button_big]
But when we define the quality of performance as a milestone, we should establish better landing criteria than stable, controlled, without losing balance and so forth. Beyond all doubt, there is research showing substantial results in biomechanical differences between groups. We know that after ACL reconstruction, maximal knee flexion angle remains decreased up to 5 years post-surgery resulting in a stiffer knee strategy during the loading phase of running (deceleration phase). This, on the other hand, may result in knee pain, recurrent injuries, or problems around adjacent joints. Similar research exists for landings from jumping.
Because most clinics involved in RTS testing are not equipped with a biomechanical laboratory—hence not able to gain significant other “qualitative details” from testing—we are limited to scores mentioned above, and of course on our ability to observe abnormal landing strategies (at least to a certain point).
Moreover, it is even questionable whether it would help the sports physiotherapist involved in the decision making which biomechanical abnormalities are detrimental. Unfortunately, the systems used to measure details in an advanced rehab stage are not widely accessible, consequently the effect of implemented interventions would not be measurable.
At our practice, Therapie Kreuzplatz in Zurich, we aren’t blessed with a biomechanical laboratory, but as a fortunate 1080 Quantum user, we were very motivated to learn from the knowledge gained from smart people around the world working with the technology. Since most potential resources and references approach performance enhancement with healthy athletes, our biggest challenge was to transfer that knowledge to the needs and goals our clients have.
Finding a way to tackle the problem of RTS clearance with athletes who have little-to-no formal background in strength training motivated us to find the most promising training interventions using the advantages of the 1080 Motion technology.
Assessing the Problem
In non-professional athletes, the athlete needs-analysis can differ enormously from client to client, as well when compared to professional athletes. Once rehab has progressed to a certain level and healing allows us to start general physical preparation, we come across a wide range of ability going from learning to squat and lunge to the immediate start on general fitness. Consequently, it makes complete sense not to rely only on time-based progression to RTS, even though it has to be considered in respecting the healing process of the graft.
In regard to the needs-analysis for the sport, the non-professional volleyball player is exposed to similar sport-specific demands as the professional player. Obviously, exposure to load in terms of intensity and volume as well as performance goals are different. Still, an essential requirement that is shared among every volleyball player independent of the performance level is the ability to decelerate one’s body weight from lunging in all directions or landing from a spike.
To successfully perform a hop test, the muscles are required to quickly decelerate and accelerate the body. Because we defined one quality criterion of the hop test by the initial and maximal knee flexion angle, our training interventions were striving for eccentric power.
Method
In respect to the stages of rehab, “pain,” and psychological readiness, we want to illustrate how we use the 1080 Quantum in order to be prepared for safely perform a hop test.
Isokinetic Strength Training
Before we start with eccentric training, we now often use the isokinetic mode to provoke an adaptation in muscle strength, since inexperienced lifters often under-load and strength gains remain limited. This appears to be the major gap to overcome when we compare professionals to non-professionals and would already increase their preparedness tremendously.
The Quantum has two main benefits in this regard:
- 1. Patients can adjust their effort to pain and psychological readiness.
- 2. The velocity limitation induces greater force production.
Playing around with different, low concentric velocities we made important observations. Usually, in this setting we would choose a specific exercise execution velocity (based on the concepts of velocity-based-training (VBT)) and would expect a certain number of repetitions possible until we visually observed a drop in force. Obviously, that is another advantage of the Quantum: direct feedback.
Videos 1&2. Athlete at Therapie Kreuzplatz performs lunges with two different velocities and loads as part of return-to-play from an ACL procedure.
Previously, when measuring a 1RM squat (speed set at 0.25m/s), we observed that our less-experienced clients have produced the same force over more repetitions than theoretically expected for a 1RM test with maximal effort. To our surprise, the load (force) they were able to tolerate for the number of repetitions was way beyond the load we (PT’s) would have given them, and also what the client would have accepted.
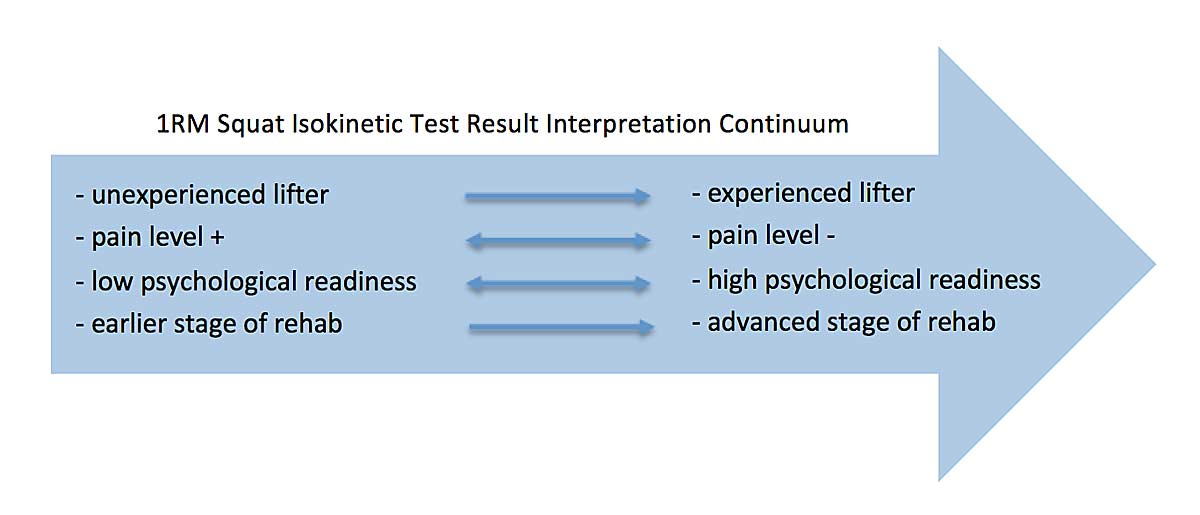
Recognizing that, we are not able to directly transfer knowledge gained from elite athletes to recreational sports participants or those with a sedentary lifestyle. The Quantum, however, helped us to discover the potential people have and gives us the foundation and opportunity—with respect to the stage of rehab—to stress them safely and appropriately. The gap from, let’s say 15 repetitions in unexperienced and 2-4 repetitions in experienced lifters until force production drops significantly, can be seen as a continuum, with the end in mind to perform a 1RM squat test as expected during an isokinetic test. Besides the experience, pain level and psychological readiness also play an important role in the interpretation of the above-described scenario.
In summary, the isokinetic mode has given us an incredible tool to work on strength and respect the client’s overall condition at any time of the rehab process. In addition, with the opportunity to do different exercises such as squatting, lunging, single-leg squatting, etc. with either the Smith machine—or with weaker clients or those with a back issue—the use of the pulley and belt system makes it even more productive for all involved parties. This definitely helps us to address the strength gap between elite and recreational to bring more clients first to a safe RTS test (such as popular hop tests) and then secondly to accomplish LSI scores > 90%.
Accentuated Eccentric Loading (AEL)
In this case of our volleyball player, since we don’t see her on a daily basis, we split home exercises and PT sessions into two different goals (at least in the early stage of rehab). The home exercises aimed to increase loading capacity towards volume (e.g., body weight), whereas the PT sessions at our facility were geared towards intensity with the isokinetic method described above.
After we reached a significant training volume and intensity without adverse effects, we started focusing on eccentrics and made use of the benefits eccentric training has to further close the strength gap and prepare the client for deceleration abilities. All of this still with our goal in mind to improve sagittal plane biomechanics.
Since we believe that eccentric power will help us to improve landing biomechanics, we use load and velocity as variables.
First, we start with a few familiarization sessions with AEL. The individual self-regulates movement velocity and we set a high ratio in eccentric to concentric load. Thereby, we rely on the concentric isokinetic force measured within the same session and work towards 80% eccentric load. The challenge here is not to induce muscle soreness or joint effusion for a week, though we also do not want to underload the athlete. This is especially challenging with clients who do not have extensive training experience or if the structural loading capacity of the knee is unknown, and therefore the reaction is hardly predictable. Consequently, in some clients, we only need 2-3 sessions until we change eccentric velocity and others need 5-6 sessions.
Once we are happy with the volume (approximately 5 sets of 8-12 repetitions) without adverse effects, we go back to bodyweight (no eccentric overload) and let the athlete learn fast eccentric/concentric movements, working towards 1s per repetition paced by a metronome.
Here, more experienced athletes often have more confidence in faster movements, maintaining limb symmetry like flexing both knees to the same degree while squatting or lunging, as opposed to less experienced clients. This has been a game changer in our mind, although we know that faster movements are important to stress passive tissue. Previously, we would have addressed these structures later in the process by hop and stick exercises, or when learning to land while dropping from a box (almost embarrassing to mention that now). Saying that, it is probably not surprising that we observe a stiffer landing strategy months after surgery when we don’t prepare our brain to trust and our structures to gradually adapt to faster eccentric contractions in an easier, more manageable task. Such important fast eccentric/concentric bodyweight exercises perfectly fit into the home program because you initially don’t need any equipment. Regarding the volume, we aim for 3 sets of 25-30 repetitions without losing speed of movement.
While our client is working on eccentric speed at home, we keep on doing AEL sessions with the Quantum. In hopes the client has adapted well to eccentric, self-regulated movement velocity up to 80% of concentric isokinetic 1RM strength, we interchangeably play with load and eccentric movement velocity.
We start with 2s deceleration, change to 1s deceleration, and in the end “as fast as possible” with one full repetition per second as the goal. With every velocity we are working towards more load with the end goal to reach maximal velocity (as fast as possible) to the load where the client and the sport physiotherapist feels comfortable. So far, we always stayed on a submaximal level between 40-80% of concentric 1RM. Of course, when it comes to “as fast as possible,” we are more daring with experienced athletes, but we are not sure about the advantages we can get compared to traditional plyometric exercises at that point.
Just as we implemented the fast eccentric speed home program, we prefer to advance to landing and jumping home exercises such as double- or single-legged drop landings, single-leg hopping etc. Once technique is satisfactory, we use the Quantum again within our one-on-one sessions in order to expose the client to accentuated eccentric absorptions. Meanwhile, the client sticks to traditional plyometric exercises in his home program, including exercises with slow and fast stretch-shortening cycles.
After familiarization with loaded landing, we are identify the optimal eccentric overload to reach maximal concentric speed in a drop jump from a small box with more experienced clients (concentric load 3-4kg, depending on the client having enough eccentric ratio available for the optimal eccentric load). With less athletic clients, we stick longer on overloaded landings and slowly advance to drop jumps; in this population, for different reasons you can imagine, we are often not reaching the point where we found a positive correlation between the eccentric overload and jumping performance.
Still, we are very focused on reaching knee flexion symmetry, since unfavorable movement patterns in the sagittal plane as mentioned earlier could have a negative effect on the individual’s health. Certainly, there are many other potentially harmful patterns, but regarding the RTS clearance and the quality criterion of hop tests we are trying to approach with this method, it could still be helpful.
What’s the Benefit of AEL in Drop Landings and Jumping?
What we have observed in the above-described scenario is that accentuated eccentric drop landings are more effective to reduce knee stiffness during running and hopping than accentuated eccentric loading without the shock absorption. Also, traditional drop jumps from different heights don’t have the same effect. In the early stages of return to running or hopping, we sport physiotherapists often observe an unfavorable movement pattern in the sagittal plane described as a stiff knee strategy, with patients describing their sensation as two wood sticks hitting each other with every step.
The benefit of AEL in drop landings, then, is that we have an acute positive response in the eccentric rate of force development and patients have an immediate impact on their running or jumping sensation, which feels “softer.”
Personally, I can only hypothesize about the underlying reason. We believe that when jumping from a higher perch our brain has access to thousands of landings and already knows what to expect. But how does our brain react when we are expecting to absorb our body…but once we have contact with the ground, we are heavier due to the amount of load we have adjusted with the Quantum? When we perform a few overloaded landings, our brain will react immediately and will adjust its muscle activation in order to protect us. The consequences for running and hopping will be that our brain will still pre-activate the same muscle potential in every heel strike, even when we are not as “heavy” as before: consequently, this allows us to feel “lighter.”
Traditionally, verbal or visual feedback cues given by sports physiotherapists are how we address biomechanical abnormalities. As far as I know, the exact adaptation mechanism we have observed is still unknown. Maybe feedforward feedback plays a role, but still in my opinion the remaining question is on how we best find interventions to unconsciously alter movement patterns because consciously we are not getting the full potential.
Where Is the Gap (If There Is One)?
As mentioned previously, there is a huge difference between a professional athletes with years of training experience reaching back to their youth and some of our regular clients. What we can learn from elite athletes is trying to stress our patients to their limits and not underload them.
With the Quantum and its isokinetic mode, we now have a tool where we can safely load our clients in all essential and imaginable directions. In addition—and probably even more important—is the potential to reduce the risk for re-injury. This is equally crucial for both professional and recreational athletes. Enough strength, sufficient eccentric rate of force development, as well as the psychological readiness may be crucial to absorb higher unexpected momentum acting on the knee. This, on the other hand, is crucial to help all injured clients for safer RTS clearance.
[av_button_big label=’Next post:’ description_pos=’below’ link=’manually,https://1080motion.com/athlete-management-sebastian-pisano-wesport/’ link_target=” icon_select=’no’ icon=’ue800′ font=’entypo-fontello’ custom_font=’#ffffff’ color=’theme-color’ custom_bg=’#444444′ color_hover=’theme-color-subtle’ custom_bg_hover=’#444444′ av_uid=’av-pu1hkj’]Total Athlete Management with Sebastian Pisano of Wesport[/av_button_big]
During our short time (15 months) working with the Quantum, although our processes with it have not been as perfectly standardized as we’d prefer, we’ve already helped many clients. Though we also didn’t apply training theory in its perfection (also due to lack of knowledge), we believe in the potential of accentuated eccentric overloading. For this, the Quantum could make a difference for future directions in rehab and return-to-sport decision-making.
Being aware that this methodological idea has not (yet) been scientifically tested, it should challenge our profession not to stick to our preferred problem-solving style. Rather, we should use new technologies to develop new methods and ideas on how we can help our clients do better in the future.
These are my thoughts, based on my current knowledge and experience working with both professional and non-professional athletes. I look forward to your feedback: please be honest, challenge me with honest critique, and help us to do better.
The above article was written by Patrick Marti, sports physiotherapist & co-owner of Therapie Kreuzplatz in Zurich. Marti received his MSc in Sports Physiotherapy from the University of Bath in 2015 after graduating as a PT in 2008. Patrick has nearly 15 years of experience as a physical therapist, working with athletes from the recreational to professional levels, and is the proud father of a young son and daughter.